Why kid’s ears get blocked easily
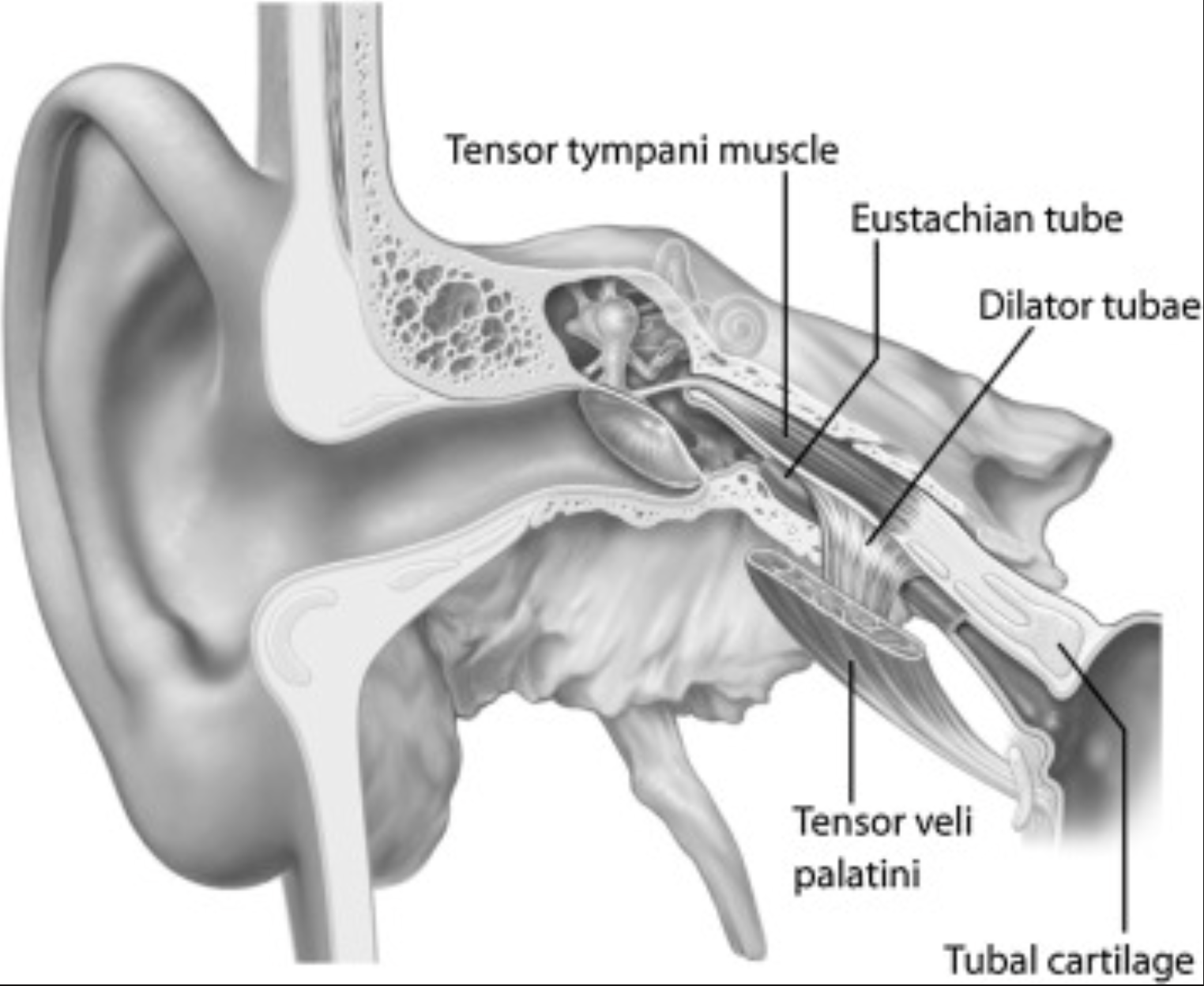
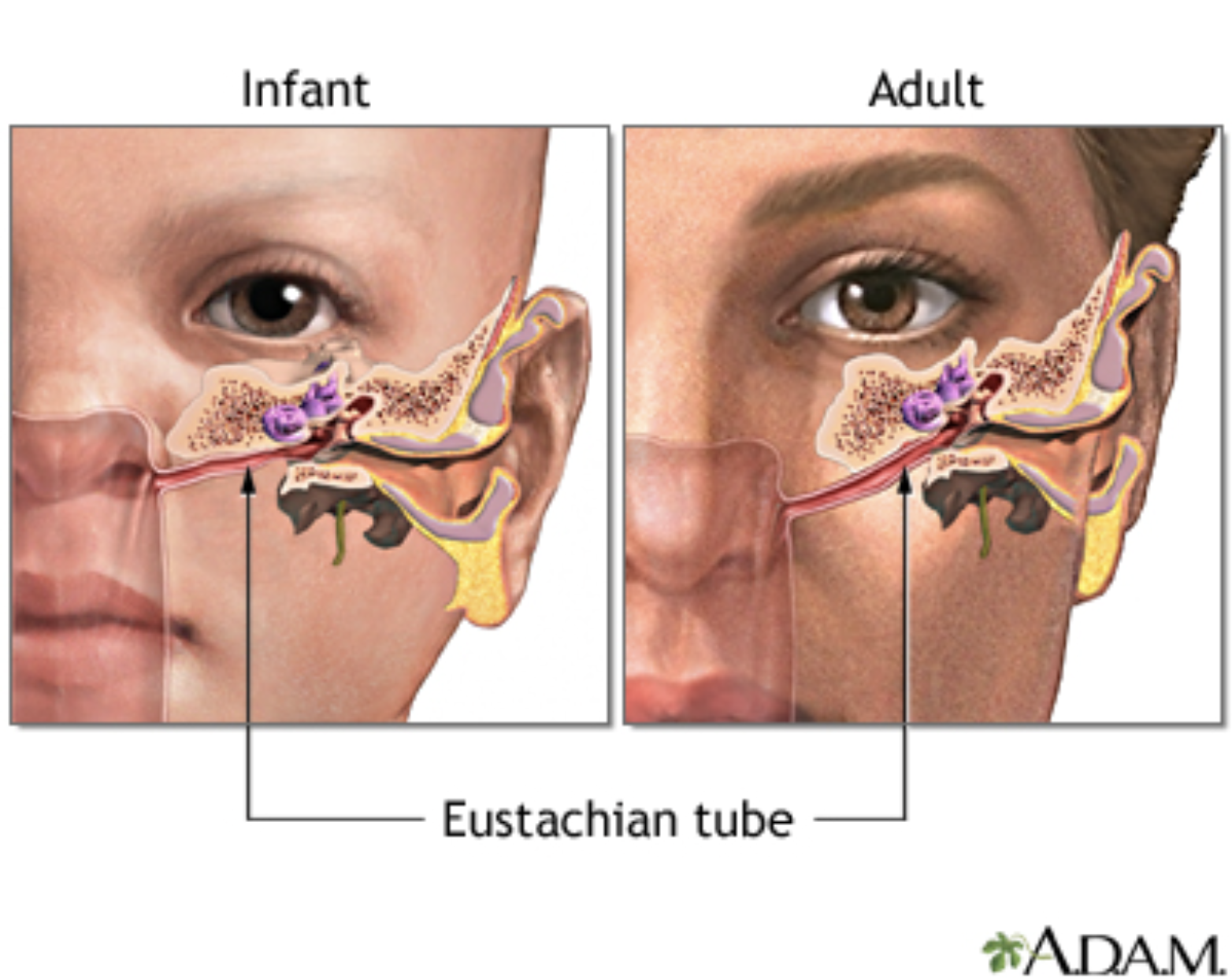
Babie’s and toddler’s ear are different to adult’s ears which explains why they seem to get very congested easily. The Eustachian tube that drains the middle ear is shorter, narrower and more horizontal in young children, so fluid and mucous can build up here instead of draining effectively.
The Eustachian tube has two roles; equalising pressure behind the eardrum and draining mucous from the middle ear into the back of the nose. When a child has a cold, allergies or large adenoids, the tissue around the tube can swell, and get blocked. They may have a blocked‑ear, “under water” feeling even if there is no infection.
This can look like:
Ear pulling, clinginess or balance changes can be from pressure and fluid, not always infection.
Toddlers and little kids being more prone to blocked ears because of their anatomy, they are not actually “sicker” children.
Eustachian Tube (Adult)
Tongue‑tie, sucking, swallowing, and the ear connection
Feeding is a great example of nature’s engineering for the face, jaw and ears. A proper suck-swallow pattern depends on the tongue being able to elevate and seal up against the palate, as the tongue drops again, it creates a negative pressure which draws the milk in and a smooth swallow.
When the tongue is restricted by a tongue‑tie, it’s functionally difficult and sometimes impossible for it to evelate well and stay in contact with the hard palate. We then see compensation with baby’s lips, cheeks and neck. You might notice clicking and gulping, inability to maintain suction, increased air swallowing and feeding just generally hard and frustrating for both mum and baby.
Over time, that lack of tongue‑to‑palate contact can shape how the palate grows and how the swallow works, which may influence how effectively the Eustachian tube opens and clears fluid.
This can look like:
“Windy” babies who swallow air easily, seem congested and noisy, or are always a bit snuffly.
Toddlers who are messy eaters, dribble a lot, or have a quite flat, “chompy” style of chewing rather than a smooth, coordinated pattern.
These patterns don’t cause infection by themselves, but contributes to the stagnation and pressure of fluid in the middle ear.
High‑arched palate, mouth breathing and chronic congestion
The roof of the mouth is also the floor of the nose. When a palate is high and narrow, the nasal passages can be narrower too, which means more resistance to airflow through the nose and a stronger tendency to mouth breathe. High‑arched palates frequently show up alongside tongue‑tie and long‑term mouth breathing.
We know from craniofacial and ear research that children with palatal and cranial base anomalies are more likely to have Eustachian tube problems and otitis media. A high palate and crowded midface can change the way the tissues around the Eustachian tube move, making it harder for that tube to open and for fluid to clear effedtively
This can look like:
A “permanently snuffly” child, dark circles under the eyes, open‑mouth posture in photos and snoring.
Recurrent “glue ear” or persistent fluid behind the drum that comes and goes with colds, even when infections are not always obvious.
There is an increased risk of ear infections (otitis media) in kids whose Eustachian tubes are not ventilating well, whether that is due to age, palate shape, adenoids or a combination of factors. The anatomy sets the stage; viruses and bacteria provide the infection.
Practical steps for parents
Get a proper assessment for tongue‑tie and function
If feeds have been challenging, or if an older child has speech, chewing or oral‑motor concerns, it is worth having a thorough assessment by people who see this every day. For example an IBCLC, paediatric dentist or ENT, orofacial myologist and a practitioner experienced in tongue‑tie and function. If a release (frenotomy) is recommended and carried out, follow‑up care is crucial: the procedure changes the structure, but exercises retrain the function.
Post‑release, we’re usually aiming for:
Better tongue elevation to the palate
Stronger cupping and suction
More efficient, less effortful suck–swallow–breathe coordination
All of these support better facial growth and may help the mechanics of swallowing on middle ear pressure.
Support tongue elevation and oromotor skills (older babies and children)
With guidance, parents can introduce playful oral‑motor work under the guidance of an orofacial myologist or speech pathologist once it’s appropriate for the child’s age and stage. This might include games that encourage:
Tongue tip to “spot” on the palate just behind the front teeth
Side‑to‑side tongue movement to lick the corners of the mouth
“Clicking” the tongue up to the palate and down again
These kinds of exercises appear in orofacial myofunctional therapy programs, which are used to restore nasal breathing, tongue‑to‑palate resting posture and a more efficient swallow.
MyoMunchee and chewing tools
For older children, chewing tools like the MyoMunchee can be a fun way to build better oral habits. They encourage:
Closed lips and nasal breathing while chewing
The tongue resting up into the palate
Stronger, more coordinated chewing patterns that support jaw growth
The current research focuses more on craniofacial development and oral function than directly on ear infection rates, but by improving these foundations we may indirectly support Eustachian tube function and reduce the tendency to chronic congestion.
Everyday positioning and congestion care
Simple things can make a surprising difference, especially in the early years:
Feeding with the head slightly elevated rather than lying flat helps reduce milk flowing towards the back of the nose and Eustachian tube opening.
Prioritising nasal breathing, addressing allergies, managing chronic runny or blocked noses with your GP, and avoiding cigarette smoke, keeps the tissue around the tube less inflamed.
Encouraging good hydration, regular movement and outside play supports overall lymphatic and venous drainage, which is part of how the body clears fluid.
When it is likely infection (and needs medical review)
Pressure, mild discomfort and some ear pulling can be part of that “congested ears” picture; infection is more likely when you see:
Fever, a very unwell child or sudden, significant ear pain
Fluid or pus coming out of the ear
A child who is extremely distressed, not sleeping at all, or not responding to pain relief
Persistent hearing changes, frequent saying “what?”, speech delay or balance issues deserve a proper hearing check and ENT review, even if you haven’t seen many “classic” ear infections.
Cranial osteopathy and ear health:
Cranial and paediatric osteopathy use very gentle, hands‑on techniques around the head, neck and upper body to support the body’s ability to balance pressure and drain fluid. In the context of ears, we are particularly interested in the temporal bones (which house the middle ear), the base of the skull, upper neck and the pathways for venous and lymphatic drainage.
There is emerging evidence around osteopathic manipulative treatment (OMT) for children with recurrent otitis media. A recent systematic review found that OMT may modestly reduce the frequency of ear infections and improve middle ear function, but the overall quality of the evidence is still low, so more high‑quality research is needed. One randomised controlled trial showed that children who received OMT alongside standard medical care had fewer acute otitis media episodes per month, more resolution of middle ear effusion and more normal tympanograms compared with children who had standard care alone.
In day‑to‑day practice, this means cranial osteopathy may:
Help ease mechanical strains around the cranial base and upper neck that may be impacting Eustachian tube function and drainage.
Support better thoracic and rib mobility, which is relevant to breathing mechanics and lymphatic flow.
Sit alongside the care from your GP or ENT – it is not a replacement for antibiotics or surgery when they are clearly indicated, but a complementary approach aimed at reducing the tendency for fluid and pressure to build up.
References
https://pmc.ncbi.nlm.nih.gov/articles/PMC12605351/
Loved this post? Pin the graphic!

This article is general information only and is not a substitute for personalised medical or allied health advice. Please speak with your GP, MCH nurse or healthcare provider about your baby’s specific situation.
Related Posts:


Learn how to differentiate between colic and reflux symptoms in 4 simple steps.
Once wound care is finished after a frenectomy, the focus can shift from structured healing work to playful oral therapy that helps your baby explore their new tongue mobility in a more relaxed way. This stage matters because babies still need practice to integrate tongue movement into feeding, soothing, and early oral development, even after the wound has healed.